
Six months into my life at Ayder, it was time to test what this department could really do. For 6 months we drilled the importance of pre-rounding, rounding, persistent patient care and most importantly, accountability. We have created a dependable, efficient and safe team. As a team, we can figure almost anything out, triage any problem and act quickly. When we can’t, we sit down and pontificate. Our collective knowledge and experience has proven itself powerful on many occasions
So, for the first week in February, we combined our mounting confidence, a safe and efficient team with the experienced hands of a head and neck surgery mission from the states (led by Dr. Terry Day from MUSC) and tackled some of the most complicated cases I’ve ever been a part of.
Our next 3 posts will highlight the 3 individuals with extraordinary pathology and I’ll try to post one each week:
-21yo law student with a massive tongue vascular malformation
-10yo with a deadly and disfiguring chondrosarcoma
-18yo with 99% tracheal stenosis after a failed resection and anastomosis in the capital



While reading this, I hope you will question our reasoning and rational. I’ve had to question my very core values of medicine and surgical management since adapting to practicing here. From a public health perspective, I’m here to teach and spread my training as wide as possible in an attempt to shape the care of head and neck pathology in Ethiopia for generations to come. But from a medical practice perspective, my typical sense of triage is broken. Although my western training teaches me to treat as efficiently as possible to affect as many as possible, I can’t do that here.
I know when I see terminal conditions like technically unresectable squamous cell carcinoma, metastatic nasopharyngeal carcinoma, metastatic sinonasal melanoma, and anaplastic thyroid carcinoma there is very little I can do surgically. But when I encounter young people with a potentially treatable disease, all my energy, time, and resources gravitate towards them. They are all suffering from the “long defeat,” a phrase I recently came across in Tracy Kidder’s Mountains Beyond Mountains.
In her story, a medical organization spends nearly 20,000 USD to fly a terminally ill child to the US from Haiti to treat metastatic nasopharyngeal carcinoma only to realize that she was past the point of treatment and died in the United States just weeks later.
The criticism is that we should be using our resources for the greater good; meaning we should treat more patients with simpler and easier pathologies. Use odds to our advantage to make the biggest impact. But many patients and these next 3 are examples of those competing in the “long defeat.” In competition with their diseases, these patients are much more likely to lose. However, I feel strongly that we can’t let them compete alone. Recruiting them into our head and neck family becomes my ultimate priority, so if they end up losing, we do it together. And indeed, for all of these cases, we are failing together in the hopes that one day we will get lucky and succeed. For whatever the definition of success is in these cases, I’m never quite sure.
So I invite you to join along and challenge yourself to come to your own conclusions while reading about these amazing people.
—————————————————————————————————–
Let’s begin with our young man with the tongue lesion. Currently a 21-year-old second-year law student, I had heard rumors of his pathology since I arrived. Yilkal and members of the OMFS team had seen him many times over the years but determined his surgery needed to wait until to “right” surgeon came for a mission. I came to learn, they weren’t waiting for me, but for someone way more experienced than me that could perform a free flap to replace the total glossectomy.
This brings up the concept of free flaps for Ethiopia. For the medical naive, a free flap is taking viable tissue with its arterial and venous supply from one area of the body and using it to reconstruct a defect while preserving its ability to circulate blood and important nutrients. Without this ability, we rely on rotating tissue still connected to its blood supply or taking small pieces of it and hoping that it creates its own blood supply using nutrients and growth factors from nearby tissue in the wound (i.e. a skin graft). From my residency, I’ve been well trained to perform any of these on the reconstructive ladder. My residency was plagued with late night flap checks, flap failure, take-backs and leeches (for when the flap gets too much venous congestion). But technical ability is only a small part of the problem. You need excellent equipment and diligent, flawless post-operative care. We aren’t ready from the equipment side and we are still in the process of prepping our ENT and ICU teams to manage these patients post-operatively. But this is a moot point at the moment, as it turns out, he didn’t need a free flap.
As you can see from the video, he suffers from a massive vascular malformation of the tongue from tip to base. The posterior 2/3rds seemed to isolate itself to the right unilateral tongue, but the anterior portion had fungated into a massive redundant malformation. You can tell from his short stature that nutrition intake had always been a problem. This was further exemplified by the complete malformation of his mandible. I can only assume from years of attempting to keep the entire mass in his mouth, he progressively developed an open bite deformity as his mandibular ramus and condyles reshaped to fit its new anteriorly displaced home.
Every time I see him release his tongue from its comfortable holding spot, I can’t help but try to transport myself into his shoes. Years of social isolation; partly from its bizarre nature, partly from an inability to communicate. He clearly diverted his time and energy to studies and when he does speak, albeit in simple phrases, he is intelligent and insightful. He is studying law with the understanding that he may never actually be able to speak clearly.
On analysis of the tongue, from the right base to anterior 1/3rd was complete with malformation, but on palpation it was superficial. Or at least it appeared to slope away from the native tongue starting from the midline. On flexible scope, it did not involve the vallecula or the lateral oropharyngeal wall. On the ventral surface of the tongue, however, there appeared to be hypervascularity of the floor of mouth, but on palpation, there was no evidence of deep disease. Putting it all together, you could take this whole thing out and just close the tongue to itself.
The great thing about the tongue is that has an amazing power to heal. Rich vascular supply and the saliva that bathes it appears to create a nice biofilm of protective bacterial, helping to prevent super-infection. So, if you can keep half the tongue, you don’t always need extra tissue. Depending on where exactly the defect is, you can just repair it to itself or slap on a full thickness skin graft. If you’re really trying to avoid a free flap, you can even rotate a submental island flap (skin, fat and muscle from the chin) pedicled to the facial artery and use it to repair the tongue and give it bulk.
Having said this, free flaps can be very useful for a hemiglossectomy repair. One of my favorite patients in residency was a 21-year-old girl who required a hemiglossectomy. Based on the bulk of her disease, her ability to speak multiple different languages and other social influences, we decided to perform a forearm free flap. Taking from her non-dominate hand, we took skin that was already decorated with a geometrically appealing tattoo. Thus, transplanting her forearm tattoo to her tongue. A feat she was very proud of.
Our current patient, also 21 years of age and pursuing a profession dependent on speech, these were also important considerations. After a lot of discussion and explanation of the procedure, his goals were to have his appearance normalized and increase functionality with speech and swallow. And, after explaining that, best-cased scenario, we would be ready for free flaps in a year the decision was to go without one. In addition, with the hands and experience of Terry Day here with us, this was the ideal time to do it.
Based on our pre-operative exam, the challenges were going to be: 1. The intubation 2. Bleeding 3. Reconstruction of the defect.
The Intubation:
Partially because of his malformed and subluxed mandible, the bulky nature of his disease didn’t fall back into the airway while supine. Since he was able to move air freely while doing so suggested that his direct laryngoscopy would provide a semi-clear shot to the larynx. This also suggested that when he is placed under general anesthesia, we should be able to ventilate(at least through the nose). And, since we were working in the mouth, a tube placed through the nose would be best. If I felt that an intubation weren’t possible, I’d ask for a flex bronch and do it awake. But, all of our collective intuition and experience suggested this should be doable. With a bronch set and scalpel on the side ready, the anesthesia team (with the help of an American nurse anesthetist that was also with Terry Day) was able to intubate nasotracheally on the first try. I yanked on the tongue anteriorly to help get it out of the way.

The Bleeding:
I had operated on vascular lesions of the tongue before. As long as you stay within healthy tongue tissue, hemostasis can be obtained slowly with careful electro cautery. This wasn’t today’s case. With a needle-tipped Bovie, electricity is transformed to heat as it is transmitted across individuals tongue muscle fibers. As the tip contacts a bundle, it will twitch, superheat, retract and then release at its center. The intense heat cauterizes each end as it breaks preventing any leakage of red blood cells. Theoretically, this mass had been present for so many years that neovascular recruitment extended deep into the native tongue. Every 30 seconds the twitch and break would be followed by a river of dark red blood. The liquid serves as a heat reservoir and thus the river’s source is spared the heat required to cauterize the vessel shut. Gentle and directed pressure is needed to slow flow long enough for the heat to accumulate. At a certain point, this back and forth of cautery and bleeding becomes unbearable. Terry and I looked at each other and all I had to say with a leading intonation was “lingual artery?” and we transitioned to the already prepped neck to explore the carotid and ligate the over-utilized blood vessel to the tongue. To make things trickier, we decided to plan for the submental island flap at the same time, so if we needed that extra bulk, we could use it.
The difficult part here is isolating the external carotid and following each branch to correctly identify the lingual and facial arteries. Since the flap would be supplied by the ipsilateral facial artery, sacrificing it could kill the flap. Problem is, quite often the lingual and facial arteries commonly branch off the external carotid together and then bifurcate. So, each branch had to be followed until it’s anatomic path made it certain to identify it correctly. The complexity of anatomy and the precision technique required to do this type of surgery is what excites me about being a surgeon. Having a chance to do this hand and hand with a legend in the field, for a terrible disease, in Ethiopia, with my very own residents, was one of the highlights of my short medical career.
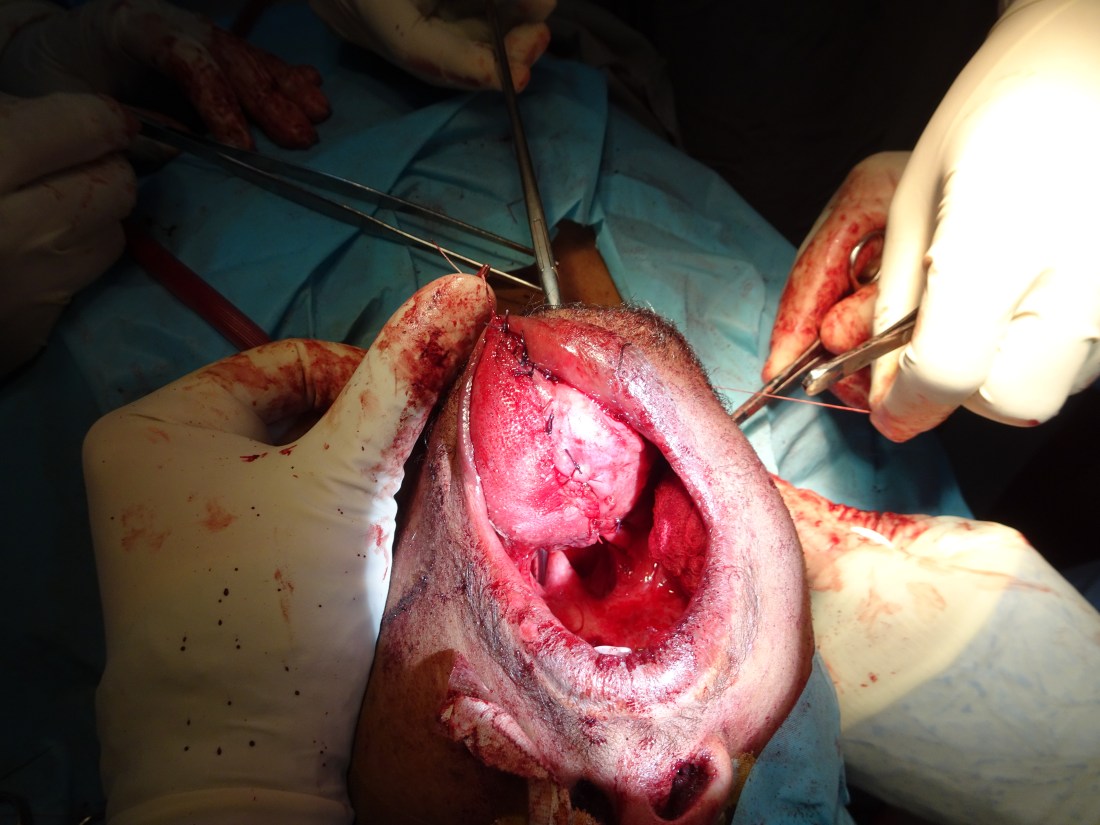
After beautiful and elegant dissection, a large, healthy submental island flap was isolated on the facial artery and the lingual and ascending pharyngeal arteries had been ligated. Literally, before your eyes, you could see the vascular malformation deflate. We were able to remove the entire malformation in less than 30 minutes. What we were left with was a hemi glossectomy defect and a partial remnant of the malformation in the floor of mouth.




The Reconstruction:
Before you decide on reconstruction, you need to consider functionality. Will he have enough bulk and motility to control both swallowing and speech? If not, which do you sacrifice to preserve the other? In his case, with the majority of the base of the tongue still preserved, as long as the food got past the oral cavity, the rest would run smoothly. Articulation, on the other hand, is tricky for him. Some if his articulation difficulty comes from his malformed mandible and a lot from his massive tongue mass. With half of his anterior 2/3rds of his tongue musculature, as long is it didn’t heal anchored to the floor of mouth, articulation would come with time. The only unknown was what would happen to that portion of the floor of mouth that harbored residual vascular malformation? If we moved on the submental island reconstruction, we would have to tunnel it through the malformation on the floor. Since its difficult to predict it’s edema post operatively, the decision was to reconstruct with primary repair. This was a simple task and was completed after another hour of work. At the same time, the other half of the team closed the neck and protected the well created submental island flap.

The reconstruction wasn’t the prettiest, but after 5 days of tube feeds, he began to take food by mouth and was discharged home to heal, recover and practice with his new tongue. His next step is to meet with the OMFS team to see if anything can be done with his severely malformed mandible (I’ll update the blog once this comes to fruition).
I’m excited to see how this surgery affects his life. Will he become more articulate and be able to express the intelligent thoughts I know are circulating in his head? Will he become more confident? What type of law will he practice? Or will this malformation recur and he be placed back at square one.
When I reflect on this, I have no idea how I’ll be able to leave at the end of July. This patient population doesn’t need me as much as I need them.
Up next; the 10-year-old with a massive facial chondrosarcoma
