
The weekend back from Addis was wonderful. Although, still recovering from a cold, Saturday was spent relaxing and then with Yilkal’s family watching the Arsenal game followed by dinner in the pouring rain with a wonderful group of people (3 American Peace Corps, 3 Belgium students, and the 4 of us). Sunday, the girls went to go swimming at Axum hotel (the place where I first stayed when I moved here), while I sat outside with a Buna and enjoyed the fully functional Axum WIFI. Well, I was only half enjoying that time because I used it to figure out how to survive here on my savings. If you’re just joining the blog: because of huge bureaucratic restructuring, there aren’t any government officials appointed to move my paperwork to be processed. Thus, I’m not being paid a cent. Clearly, I didn’t come here to make money, but I wasn’t expecting to live off my savings, so I have to move some things around.
OK, enough about that. After Axum, we met with a large group of Spanish people from Wukro (a town about an hour drive north) who are volunteering at an NGO for a couple of weeks. We had a wonderful lunch and spent the entire afternoon at a milk/pancake shop with a hilarious name (see picture).

Randomly and bravely, an American girl in her 20s walked up to us and asked to join. Turns out, she just finished NP school and is taking 4 months to travel eastern Africa BY HERSELF. It was fascinating to listen to her stories. I had a very basic understanding of how difficult her life must be, but I really had no idea. I hope the rest of her trip goes well.!
My week back at Ayder was ramped up to full speed. I didn’t have time to think about my lingering illness, or troubles in Addis the week prior. Ayder gave me exactly what I needed, intense medical problems and ample teaching opportunities. In the morning the residents impressed me with their updated rounding list and formal presentations of patients. They make me proud!
The rest of the morning was spent bouncing between my office (writing exam questions for the medical students) and consults in the OPD. In that morning we scheduled our first thyroids (2 in fact), a branchial cleft cyst in a 1.5 year old, and a septoplasty (the seniors wanted to learn how to do them properly). Monday night I prepared a powerpoint “operative atlas” for the basic septoplasty for the residents. I plan on making these for all the new procedure they do.
After rounds on Tuesday, I joined Betty (one of the seniors; remember attendings are called seniors here) for a pediatric tonsillectomy and the septoplasty. I walked one of the R2s, Dessa Nicknamed “Chula” after a spatula (no idea…), through a proper electrocautery tonsillectomy which he performed extremely well. By the way, without suction bovies, we will still perform adenoidectomies with an adenoid blade. Its fast and bloody, but the bleeding stops by the end of the tonsillectomy. I’m also encouraging all the seniors to stop giving post operative antibiotics and use more than just paracetamol for pain. But, I must say, all the Ethiopian children look amazing and lively on post-op day 1.
The septoplasty was a difficult one (as everything seems to be here). The septum was completely deviated to the right caudally and then flipped back towards the left with huge bony spurs. I walked the senior through each step and although we lacked sharp instruments, a swivel knife, anything long enough to cut bony septum from the cribriform, or proper suture, she performed well with a great strait septal result. During the middle of the case, I introduced the endoscope to really highlight the deep anatomy which really seemed to click with everyone. Septoplasties can be very difficult and stressful, but I was excited to teach new procedures and techniques. This case was a perfect example of why I’m here. I was happy (as you can tell from the pictures).



I then broke off that team and took Chula with me to debride our well-known neck wound again. We together dissected off the necrotic IJ and carefully debrided necrotic tissue from the strongly pulsatile floor of the wound. Knowing at any second, the carotid could blow in our faces. Well, it didn’t and we moved on to clearing tissue from the parotid, down to the mastoid tip, styloid and transverse process of C2. This infection had gotten everywhere, but for the first time, we were getting ahead of it. We sent tissue for culture, irrigated it out and switched to wet-to-dry dressings. It was going to be a long-game to fix this infection and wound, but I still didn’t feel comfortable placing fresh tissue on top. He isn’t ready. Once the cultures come back, I’ll narrow the antibiotics and consider decannulating him. I’m amazed he’s alive and I still have no idea what actually happened here. The two white parts you see in the wound now are the exposed thyrohyoid membrane and the angle of the mandible. And… a tiny bit of purulence left over around the mastoid tip.



That afternoon I was in the OPD and was presented two unique problems. First was a guy from my initial week here. I’ll repost his CT scan for you as a reminder. He had a terrible cholesteatoma that resulted in a bad infection dissecting through his lateral mastoid cortex and into under his skin. We completed a canal wall down mastoid and resected dead skin and closed, but 3 weeks later he presents with a posterior defect. Luckily, the mastoid bowl deep to it seems intact and healing. So all we need to do it close the defect with a nice little local tissue flap. There are two procedure beds next to the OR for minor procedures done under local. I walked Chula through a rotational flap and he did a great job! As you can see (this was actually done the day I write this post, but who cares).
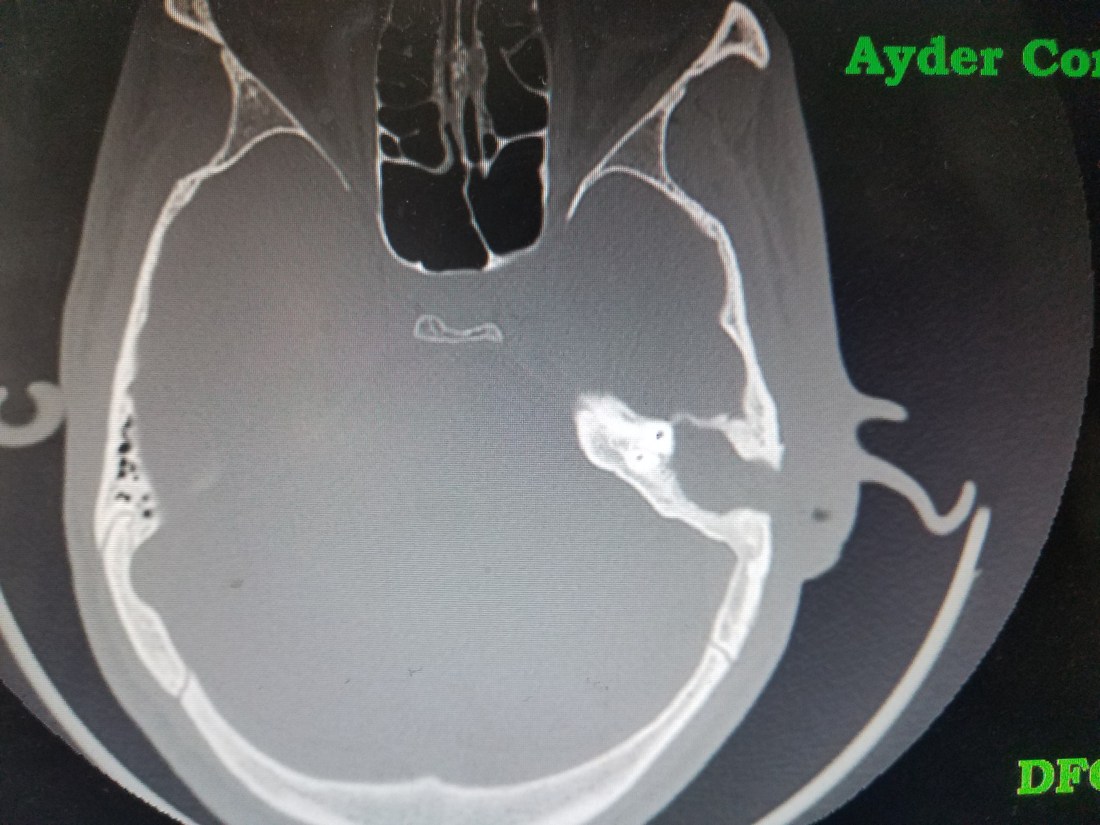



The second problem reminded me of a case I saw in residency. This was a 20yr who suffered road rash in a car accident that actually completely avulsed his ear. He was asked to come to our OPD to consider an auricular reconstruction, but my mind immediately when elsewhere. If the ear was avulsed and the scar covered his canal, then the skin in his external auditory canal (EAC) be constantly reproducing itself with nowhere to go, forming a cholesteatoma. There wasn’t anything obvious on the skin and I really had no idea what his temporal bone or middle would look like, so I had him obtain a CT. Wouldn’t you know, it shows a big cholesteatoma in the EAC, but a perfectly intact temporal bone, middle and inner ear. I reached out to my favorite Otologist in the states (the one who had a similar case in my residency) and he agreed with me and encouraged me to recreate the EAC. If we were able to do so, we might be able to restore some of his conductive hearing loss and make his standard of living significantly better. These types of cases are exciting because they present new and challenging dilemmas with potentially excellent benefits. Not to mention that if we didn’t fix the problem, the cholesteatoma would eventually erode into the mastoid, middle ear or intracranially and cause some significant problems. So, we will add this to the never ending list of patients waiting for the OR now.

That night I had an interesting consult. It was a 4yo boy who had been intubated and on a respirator for 20 days recovering from Guillain-Barre syndrome (GBS). Now, of course I learned about this in medical school and have been always aware of it, but this was now the second patient I’d ever seen with it and both were in Mekelle in the past month.
GBS is considered to be a type of immune-mediated disease associated with ascending paralysis leading to respiratory failure. The theory is that after an infection with an array of minor illnesses (like campylobacter jejuni or CMV, EBV, etc.) the body produces antibodies that are very similar to glycolipids found in myelin of the peripheral nervous system. So, weeks after the illness, lymphocytes infiltrate spinal roots and peripheral nerves while macrophages strip myelin from them, disabling the conduction of nerve impulses. Recovery occurs only when the attack stops and the myelin regenerates. E-medicine has a great outline of the disease if you want to learn more.
The first patient we had was an older gentleman that our team trached about 3 weeks ago. He still hasn’t recovered. This boy, on the other hand, had started to get better. He was spontaneously breathing and had full facial movements. The ICU had tried extubating him twice before (the last time was ten days prior). I suggested to them a trial of extubation steroids and one last extubation attempt. They did so and the extubation attempt the next morning failed. When I tried to ascertain how he failed, I could tell that the concept of subglottic stenosis and stridor induced failure was not on their mind. Nevertheless, the failure was apparently immediate and obvious. A tracheostomy probably should had been performed a week ago, but now was certainly the next best choice. Without a pediatric cuffed trach, the plan was to place a 5.0 PEDs Shiley and really hope that the leak around the tube was small enough to still allow for good positive pressure ventilation.
According to our textbooks, when respiratory failure occurs, the average time on a vent is 50 days and 80% walk independently at 6 months. Even with good tertiary care in the states, mortality rates can be from 2-12%. The best chance this kid has of surviving is getting a trach, getting off the vent and out of the ICU. If he could make it out without developing a hospital/ventilator acquired pneumonia then he could wait the time necessary to recover and possibly be decannulated. The other potential problem was how much damage did his 20 days of intubation with a cuffed endotracheal tube do to his subglottis?
Although the case was delayed for 2 hours because they ran out of sterile drapes, it otherwise was extremely smooth and fun to walk the residents through the case. We began with a bronchoscopy which showed, unfortunately, really aggressive ulcerization and injury to the subglottis (probably a big contributor to the failure to extubate earlier). The airway was otherwise normal. The tracheostomy was completed with ease and he ventilated well with the cuffless 5.0 PEDs shiley. We shipped him back to the ICU in stable condition. Just 4 days later he was ready to wean to CPAP and will hopefully get off the vent soon.

Although I got home a little late, Jon had prepared a traditional Spanish meal for one of their Ethiopian friends that was leaving for Europe soon. Equipped with cheese and meet brought over from Spain, this was by far one of the best meals I’ve had in Ethiopia.

Jon and Alaine even convinced me to try something else classically Spanish, apparently. Although they claim they have it all the time…they may have just been messing with a naïve American. They claimed that mixing red wine with Coke (yes, the soda) was a normal thing they did back home. I tried it; for those of you who know me, you can tell how I feel about it from my face.
This was a great meal to prepare me for the next day. I will dedicate an entire post to this soon, but it was a 10 hour marathon and the hardest surgery I’ve ever done in my life. It was an excellent team effort and very successful. I’ll give a sneak peak of it now, but it deserves its own post once I get the final pathology back.




Friday was spent recovering from the prior day with seeing patients in clinic and enjoying afternoon seminar with the residents. In the afternoon, Alaine and Elisa were going trekking with the Spanish people from the beginning of my post, but I was just far too tired to make the journey. Not to mention that I was now pouring copious green purulent mucous from my nose every 5 mins. Given that it was 14 days into my illness, I was still spiking fevers and my head always felt like a balloon, I pulled the trigger and started augmentin to treat an acute sinusitis. Given the week I had and the one I know I have coming up, a weekend of trekking seemed daunting. It was a good decision not to join.
Next week I have a full line-up of interesting cases, but of course, I will leave you with puppies :).

