
The culmination of today’s events warrants its own post, breaking from my normal chronology. Today did mimic other Mondays with its clinical burdens, but I feel the need to express what occurs in a day in the life of a head and neck surgeon in Mekelle.
Sorry, not many pictures in this post, but next week I’ll update most of these stories with pictures.
For context, last week we decided to reach out to the members of the American Academy of Otolaryngology to encourage collaboration for what we are accomplishing here in Mekelle. The outpouring of support we have received has been more than I could have ever imagined. For those of you who are new to the blog as a result of that posting, welcome. The support of the head and neck community has surfaced a huge array of new possibilities and on my ride to work in the morning, my mind was racing. The driver of the morning van, Ashinafi could sense my pensive state. Ashinafi is no master of English, but he knows enough to express his innate ability to analyze human behavior and to be introspective. We often talk about human nature and why people do terrible things. I didn’t know these facts at this particular moment, but this morning brought in reports of at least 23 people being slaughtered on the outskirts of the capital. Some Ethiopian news reports even suggest these attacks were ethnically driven and this was a systematic killing of certain groups of people. Ashinafi, in his Gandhi-esk, infinite wisdom, minimal vocabulary way said, “Do not start your day with a heavy mind or you will not do good.”
As with a lot of our conversations, I could have completely misunderstood him, but I think he was right. Regardless of how much work there is to do or if the world around you seems to be falling apart, you must clear your mind before performing your job. You can’t bring the weight of yesterday to today’s work or else “you will not do good.” His slightly ambiguous phrase worked and I walked through the always-open front doors of Ayder Hospital ready for what was in front of me. I couldn’t have predicted what this day would be like, but at least I was approaching it with a clear mind.
My first task of the day was a lecture to the department to standardize the workup of thyroid-related disease based on our latest guidelines. Since my arrival, we’ve decided to open our doors to thyroid related issues in order to help relieve general surgery of this unnecessary burden and to enhance our department’s breadth of care. On the way, I pass the hallway of the Emergency Department and as always, silently scoff at the sheer volume of patients crowding the hallways waiting for attention from the medical staff.
A quick walk through the inner courtyard of the hospital, a left at radiology, just past the HIV/AIDS specialized pharmacy, I arrive at the pathology conference room where we often hold our conferences. During my lecture, I’m always amazed at the eagerness of the residents. Eyes locked on me, carefully listening to every word, taking the mental energy to translate it internally and breaking gaze only to write something down they consider vital to remember. I know they must concentrate on me that intently in order to understand what I’m saying, but it adds to my joy of teaching. I can’t imagine trying to learn complex treatment pathways in a foreign language and its another example of just how intelligent these residents are.
After the talk, Seid comes up to me to tell me about a patient in the ER. He doesn’t miss a beat even despite half his face being consumed by angioedema induced by a bee sting the day before. With one eye on me, and the other half-eye navigating the periphery of our walking path, he describes an 11 year old who was carrying water to the family house when she went missing for a couple of hours. She was found down by the family with the rope of the water bail across her neck, breathing, but unconscious. He family brings her into Ayder 4 days after they found her down. She remained unconscious throughout this time apparently. We were consulted to rule out cervical trauma. Seid informs me that there was no stridor and no difficulty breathing on room air. Even though this probably wasn’t an airway issue, the story warranted our immediate attention. I took him and Fili (our only female resident back from holiday) to the ER with me to figure this out.
Entering the ER hallway, past 3 guards simply there to keep the volume of humans to a barely acceptable level, we elbow our way towards the pediatric section of the hallway. A young woman in a pristine white coat catches my eye. I trace up the white coat to her face which wore a face I myself have worn before; paralyzing panic. I followed her line of sight which met her hands pressed firmly on the chest of an infant laying lifeless in the lap of his mother. As I witness the actions of her hands compress the sternum inwards towards the cervical spine, my attention turns to the mother who is holding her baby. The mother’s fear has disassociated her from her surroundings as she stares blankly into the ambient air, rocking back and forth, sobbing.
Realizing that this is likely an intern (all residents go to morning lectures in departments all over the hospital at this time of day leaving rotating interns to cover the entire hospital including the ER, ICU and PICU), I grabbed the baby from the lap of the mother and placed him on a nearby already occupied stretcher. Seid took over the job of attempting to create manual blood flow throughout the body while I asked the ER intern where the code team was and where the intubation supplies are located. She had no idea, she probably just started her rotation there today and this pulseless, lifeless baby was her orientation.
I told them to keep going and I sprinted upstairs to the office where I stash pediatric airway supplies. In less than 60 seconds I’m back and place the 4.0 uncuffed endotracheal tube like I have done hundreds of times before. This, however, was my first placement into an already deceased infant. Seid stopped compressions long enough to me to confirm pulselessness and for the baby to perform a seemingly purposeful attempt at an inspiration only for me to realize that this was the brainstem’s last-ditch effort for survival. While providing ventilation, leaning on whomever the other dying patient was sharing this stretcher, I look up to see the ER intern watching us. I demanded the code team and for the proper people to take over this code from us bystanders who should be the last people running the code.
Well, I don’t know why I didn’t assume this already, but there is no code team, nor an organized method of reviving a pulseless infant. I had no idea how long this baby had been pulseless, but I knew he had no chance. I watched as the ER team attempted to place epi through a clearly clotted IV line and after several rounds of CPR brought no return of electrical activity, I watched as the team rolled the baby in the blanket he was laying in and stepped back to allow the grieving family to regain control of their baby that simply had no chance to live in this world.
We were forced to turn our attention to the task that brought us to the ER in the first place. The young girl found down. 3 feet away from the previous scene is a room in the ER designated for pediatric care. Passing through the doorless doorway the entire room is littered with children of various ages and illnesses linked together by identical strands of plastic to a centralized IV pole. Amongst the deafening wails of a dozen children, we ask the nurses for the location of our strangulation child. After about a half dozen conversations in Amharic, it was clear that no one knew. A mother of a clearly terminally ill child spoke up to indicate that the father took the child and left for home, frustrated with the lack of care. Now, I don’t really know what message that sends to me or you, but the parents of a child who has been unconscious for 4 days decide to leave the hospital to fend for themselves.
I left the ER in shock. And slowly made my way to the clinic. Perhaps good patient care could take my mind off of what had just happened. But, before I had the chance to see a patient, Bini tells me that the family of our gigantic neck necrotizing fasciitis guy that we spent the last month nursing back from the brink of death was MISSING. Bini heard from the family that he had developed unilateral weakness while driving and then left home and hadn’t been seen for over 12 hours. I imagine that his infected exposed carotid either dissected or formed a clot and he suffered a stroke. I don’t know where he would possibly go after that, but I fear the worst. May he went to visit a holy water site or receive local care, I don’t know. Did I make a mistake to send him home?
My mind was lost in emotions and I needed something good to happen…..not today.
My first patient was a 30 year old who we had just diagnosed with T4a nasopharyngeal carcinoma 2 days prior. Today’s visit was to schedule a biopsy and to explain the diagnosis. Through Bini’s translation, we explained that he had to pack up, leave Mekelle, drive the 16-ish hours to the capital and undergo weeks of chemoradiation in hopes of buying himself more years of life. His response is the same he apparently gave two years ago; he can’t afford to travel and get that treatment in Addis. Not to mention, I was asking him to drive into an area that currently has active ethnic killings by a people that have nothing kind to say about the people in Mekelle’s region. He goes on to explain that with the presence of a new western doctor, he had faith that surgery would be his best option. We will see what we can do about funding his health care, but as for the social constraints of his travel, I don’t know what to say. I don’t blame him.
2 or 3 patients later presents a well-dressed thin 52 year old male presented with a new neck mass and a left cranial nerve VI palsy (he cannot turn his left eye to the left). He came from another city with a CT in hand with a report read as normal. One brief look through the non-con axial cuts of the CT revealed a sinister appearing asymmetry in the left nasopharynx reaching up into the skull base causing local bony erosion. He had bilateral 2cm level 2 lymph nodes that were as hard as a rock. A handwritten FNA report read “suspicious for carcinoma.” Our flexible scope of the nasopharynx had nasopharyngeal carcinoma written all over it. My Wednesday that was free of OR time was now dedicated to obtaining definitive diagnoses to convince 2 young men to put their lives on hold, travel to an extremely dangerous area to obtain treatment toxic to their bodies in hopes of maybe saving them.
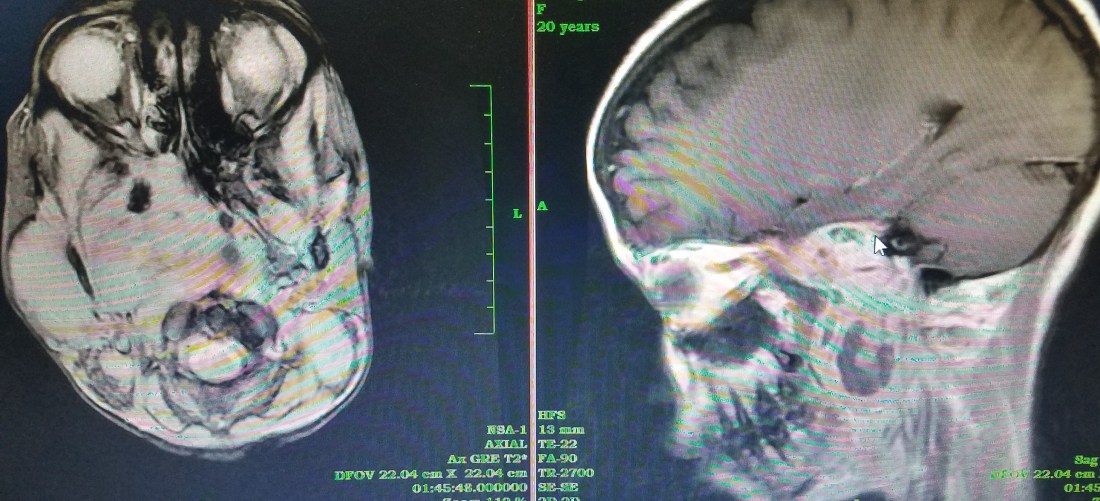
Just then, and I’m not exaggerating timing, one of the docs from the Oral-maxillary team comes in asking me to see a patient with him. He brings in a 20 year old girl with a proptotic right eye but covered by lid ptosis, a right parotid mass and a large left neck mass. He pulls up an MRI showing a large right parapharyngeal mass extending through the skull base into the intracranial space, obliterating the cone of the right orbit on its way. Without knowing for sure what this could be, I decided to take an excisional biopsy from the neck and the parapharyngeal mass through the soft palate and the nasopharynx. We will schedule this soon. Whatever this is, it looks aggressive and is in a bad space. I’m not sure what to predict for this young girl.
As the day continued, we cleaned and debrided the destroyed pinna of an inmate (that we won’t be able to see again for a month because the jail is 300 km away), booked a dozen more surgeries and met two more interesting patients.

The first was a 21 year old girl with a very large hard palate mass. The con-CT with only axial cuts (they couldn’t do coronal or sagittal recons for some reason) showed a vascular mass with a partial erosion of the hard palate. Scope of the nasal floor shows no overt communication with the oral cavity or mass. This thing clearly has to go, but will leave a large palatal defect….the reconstruction tree will be the real challenge. I called the same oral-maxillary guy who tells me he can make an obturator for me. Awesome!

Finally, one of the more difficult cases of the day. A man in his 50s that had been apparently beaten up 6 months ago was now presenting with profound left sensory neural hearing loss for 1 month duration. Fili presented the story to me and appropriately questioned its validity. The audiogram that was just performed showed absolutely no responses in the left ear and perfect hearing in the right. Now, its certainly possible to have profound SNHL following trauma, but to have it occur 5 months after the incident didn’t make sense. I had Fili ask “if you have hearing loss in that ear, how would you like us to help you with it?” Expecting to hear something like, help getting a hearing aid, or assistance at work, he pulls out a piece of official looking paper that Fili explains to me is from the court office. It requires a statement from the physician confirming his sudden profound hearing loss.
Both Fili and I were more suspicious now. Because we don’t have a 2-channel audiometer nor two tuning forks of the same frequency, we had to improvise a way to see if he had non-organic hearing loss (faking it in other words). We placed the bone conduction device on his left temporal bone and blasted a tone at 2Khz @70dB. To our unanticipated advantage, playing this tone resulted in an audible tone presenting in the entire room in which everyone could hear. Because his hearing in the right was so good, not only should the skull shaking tone presented to his “bad” ear shake the cochlea of the right (and produce audible sound), the tone presented in the room was easily 30 dB and his right ear should have picked it up. However, even though everyone in the room could hear this tone and his good right ear was exposed to it, he claimed to hear nothing. This is essentially the principal of the Stenger Test used to isolate non-organic hearing loss. When the same tone is presented to each ear, the louder tone will be perceived by the brain as the only tone. We presented the louder tone to the left ear in this case. If he were indeed completely deaf in that ear, he would have heard the softer tone in the room and claimed to hear something in his right. But since his hearing is normal, the only sound he could hear was the louder one in his left ear. AND since he was trying to claim deafness in that ear, he remained silent and said he heard nothing.
I am far from an expert audiologist, but that was enough for me to be uncertain of his hearing loss claim. Thus, I told the residents to document our findings and to not confirm hearing loss on his official paperwork. Nevertheless, I took down his phone number and told him I would speak with audiology experts in the states to either confirm our science, or to offer another way to test him.
This was my only “win” for the day and it resulted in me blocking an older man from getting money from the government. I truly believe he was trying to deceive me, but I still feel guilty.
With this exhausting day, I returned home to make pasta with salt and olive oil and to write this post. “A day in the life” normally has a positive connotation. Today was a challenge, to say the least.

One thought on “A Day In The Life…”