
Quick update: The gentleman from my Cutting Through Black Bubbling Blood post came back to clinic looking healthy as ever! His septal abscess had healed and his life-saving slash trach had left behind a very tiny scar. That 2cm scar will always be a reminder of one of the scariest times in my life. I was elated to see him and he was all smiles (in his shy/Afar way).

Also, in the next couple of weeks, I’ll be posting the story of our unfortunate Afar lady who was attacked by a hyena and suffered a substantial aerodigestive injury.

Now on to Today’s post:
Ayder hospital is the referral hospital for all of the Tigray region (and more); we get a lot of trauma. Luckily, there are a couple of very capable maxillofacial surgeons that handle all the facial fractures. Which is great, because I feel that I had more than a life-time’s worth during residency. This leaves us the complex plastics-related soft tissue, skull base, and airway-related trauma.
So many of Mekelle’s streets are handcrafted with thousands of cobblestone. It makes for really beautiful streets and sidewalks, but when up-rooted or discarded, they become an ideal projectile for irresponsible youngsters. Soft tissue injuries from these otherwise beautiful stones represent the majority of traumas we see. As such, we will review a few here. But, lets start with something relatively rare in Ethiopia; a gunshot wound.
On a Saturday morning a few weeks back, I made my way into rounds with the residents. On my arrival, they immediately diverted me into the dreaded, overcrowded emergency department. We gently elbowed past patients and their families attempting to navigate the narrow hallway towards the entrance. Turning the corner, we enter an isolated 10×10 foot room I had never seen before. Since arriving at this hospital, I have learned to look down as I walk. Hazards come in many forms, but bodily fluids are common and my shoes are dirty enough. So, as I walk into this semi-isolated box, the pool of bright red blood on the floor catches my eye first. As a few small aliquots fall from above and assimilate into the foot-level collection, my eyes trace up to the source. A breathing, but an otherwise lifeless adult male is lying prone in a pool of his own blood on a black, bare stretcher. There is no one else in this room. There are no monitors but his chest rise reassures me. I hear stertor, but also plenty of air movement.
Honestly, a bit confused by whats going on, I ask the residents for the presentation. What I hear is that this unfortunate male was the victim of a shooting 8 HOURS AGO and has been sitting in this little 10×10 cell for 6 of those hours. These days I don’t even waste my time trying to get an explanation for why I’m just hearing about this patient or why this patient has been left here to slowly bleed out over the past 6 hours with no attempt to protect the airway with intubation or stop the bleeding. While the residents talk, I put on gloves and survey the patient’s injuries.
I take down the haphazardly placed gauze and notice a large submental soft tissue injury and a clean, self-cauterized injury medial-superior to the right eye. He has slow, active bleeding, labored but patent breathing and wakes to stimulation enough to push me away. I clarify the story that someone shot him from distance which suggests that the small wound medial-superior to the right orbit is the entry wound and the submental large defect is the exit as is classical teaching. The trajectory of this made little sense, but I had a case in residency of a guy running away from a shooter that was hit (with one bullet) in the face and penis. So, I didn’t really think twice about the story, not that it mattered right now.
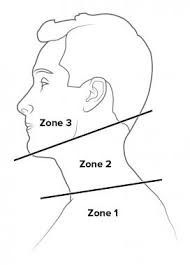
One of the first things I did here for resident education was to rewrite the didactic curriculum. For the first block of lectures, I decided on head and neck emergencies. The second lecture, of which, was penetrating injuries. We had this lecture just 1 day before this gunshot victim presented. Now, feeling as if I had somehow cosmically induced this pathology, the residents reviewed the basics. The neck is divided into zones 1-3 and each have intricacies of diagnosis and management. This gunshot involving the submental area places it in zone 3 which extends up to the skull base. This is a particularly challenging area to manage as it is full of large, important vessels and is the beginning of the airway. Thus, when someone presents with a penetrating injury to this zone, airway takes precedence (as it usually does).
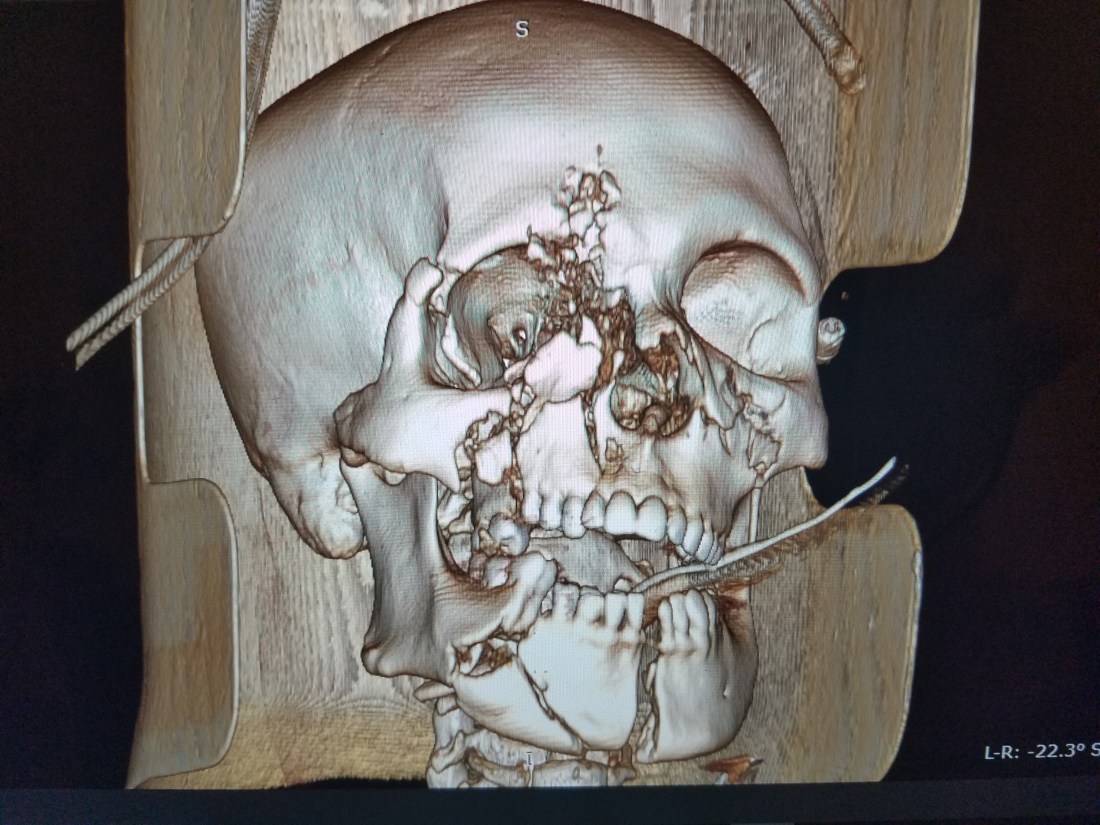
Our victim, although with loud obstructive bleeding, was moving adequate air on auscultation. Nevertheless, he had lost a lot of blood, his mandible was shattered into pieces, his floor of mouth was obliterated and his anterior 2/3 of his tongue was macerated. Not to mention a large hole in the hard palate with a half dozen maxillary bone fragments arranged in no certain evolutionary pattern. The key to his survival over the last 8 hours has been the preservation of his base of tongue and oropharynx. If remaining prone, his blood would escape to the body fluid-soaked floor of the emergency room and leave his airway patent. Moving to supine would force all of the oral cavity elements into the oropharynx and obstruct his airway. We need to keep in mind here that under ideal circumstances, he would have been intubated on arrival and the airway checkbox would have been completed hours ago.
Since his airway was patent for the moment, we move to the next checkbox of zone 3 injury. Hemostasis. With a plethora of compact, vital vasculature encased by thick bone, bleeding here can cause brain death (from anoxic injury), exsanguination, or loss of airway (from liquid asphyxiation or obstruction). Although lethargic, he was following commands and the bleeding was a slow trickle at this point. A quick palpation of his right radial artery confirmed tachycardia. His tachypnea, paleness, and fatigue all suggested severe anemia. There was no blood in the hospital at this moment, so he had to work with what was left intravascularly.
It was clear to my residents and to me that he was severely overdue for an endotracheal tube. It was at this moment that our maxillofacial surgery friend presented, a bit worked up and anxious. He palmed a laryngoscope and was planning to intubate right here and now, in this blood-soaked, dark, 10×10 room. Otolaryngology, Head and Neck surgery in Ethiopia does not have the reputation for being airway experts, but our training in the states and my pediatric fellowship has equipped me with a knowledge and skill base uniquely fit to manage the most complicated airways.
So, I received the normal distrust from all involved when I suggested that this gunshot victim’s airway was patent enough to wait until we could roll into the OR and have all the equipment, anesthesia, space, light, and dry floor to perform a safe intubation.
Even though the emergency OR was literally just 10 feet away, the process of rolling him there took 30 minutes. After securing an airway with ease, we placed a trach and then worked hand-and-hand with the OMFS team to repair the neck, floor of mouth and stabilize the facial skeleton.




After seeing the wounds and again analyzing the CT scan, it was now clear that this was a self-inflicted GSW with from the submental area up. Just like portrayed in the movies, I believe he attempted to commit suicide with his head in extension and the pistol under his chin. Contrary to a high-velocity missile impact from distance, a close-range shot creates a large pressure wave at its origin resulting in extensive soft tissue injury that funnels down into a less destructive pressure wave. This method of suicide is usually unsuccessful as vital brain structures are spared and only soft tissue of the head and neck are injured. If the bleeding is controlled and infection prevented, survival is likely. In fact, a month after his presentation, he was decannulated and transferred to a military hospital.
What we lack here in Mekelle is what he probably most needs. Good psychologic counseling. I’m curious what will happen to this man, but I’m worried I will not see him again.
Now, switching to cobblestones. For whatever reason, this is the weapon of choice for the young population. The inertia these stones carry is far too much for the bones and soft tissue of the face and they give way easily. I’ll let the pictures speak for themselves, but I’ve been teaching my residents to not only focus on aesthetic repair but also functional. There have also been some massive crush injuries to the nose that we will reconstruct with the help of a facial plastic surgeon visiting in January.




Next most common pathology for trauma is motor vehicle accidents with various forms of head and neck trauma. Again, no need for words here…






Finally, we encounter quite a few blunt traumatic injuries to the larynx. They usually come in the form of strangulation with the arm or hands. Throughout my training, I really didn’t see much of these injuries especially compared to the half dozen I’ve already seen here. The initial assessment of these injuries requires the evaluation of the airway. If the flexible laryngoscope is clean and the patient is asymptomatic, then no further workup is needed. That’s not how we receive patients here. Each one presents symptomatic, from dysphonia to stridor to respiratory failure. Laryngeal hematoma was an extremely rare finding in my residency, but very common here.
Thus, those patients with blunt injury to the neck that are symptomatic and have findings on laryngoscopy, we have been obtaining a CT. According to best practice, if the CT reveals depressed fractures, a strong consideration should be made for reduction and repair. In two such cases, we encountered a young male with dysphonia, mildly increased work of breathing, glottic and subglottic hematoma and a CT finding of a depressed segment of anterior cricoid.
One of these individuals was progressively worsening so we proceeded to the OR only to find him in a hypertensive crisis. Since anesthesia and intubation was not an option, we proceeded with a reduction and repair of the cricoid under local. I thought to myself, I’ve been a part of countless awake medialization thyroplasties and awake trachs…whats the difference? It ended up proceeding very well and we used tiny titanium mesh plates to keep it reduced. With real-time feedback, he had an immediate improvement in voice and work of breathing. An interesting experience.

The other individual presented 4 days after the injury and was slowly improving. We decided to treat him conservatively and not proceed with the repair. I’ll follow him closely to watch how the subglottis heals.

One thought on “Trauma In Mekelle”